Product Detail
Product NamePKHD1 Antibody
Clone No.A1-G12
Host SpeciesMouse
ClonalityMonoclonal
PurificationProA affinity purified
ApplicationsWB, ICC, IHC, FC
Species ReactivityHu
Immunogen DescRecombinant protein
ConjugateUnconjugated
Other NamesARPKD antibody
FCYT antibody
Fibrocystin antibody
FPC antibody
PKHD1 antibody
PKHD1_HUMAN antibody
Polycystic kidney and hepatic disease 1 protein antibody
Polyductin antibody
TIGM1 antibody
Tigmin antibody
Accession NoSwiss-Prot#:P08F94
Uniprot
P08F94
Gene ID
5314;
Calculated MW445 kDa
Formulation1*TBS (pH7.4), 1%BSA, 40%Glycerol. Preservative: 0.05% Sodium Azide.
StorageStore at -20˚C
Application Details
WB: 1:500-1:2,000
IHC: 1:50-1:200
ICC: 1:50-1:200
FC: 1:50-1:100
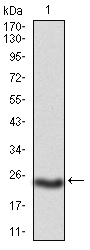
Western blot analysis of PKHD1 on mouse PKHD1 recombinant protein using anti-PKHD1 antibody at 1/1,000 dilution.
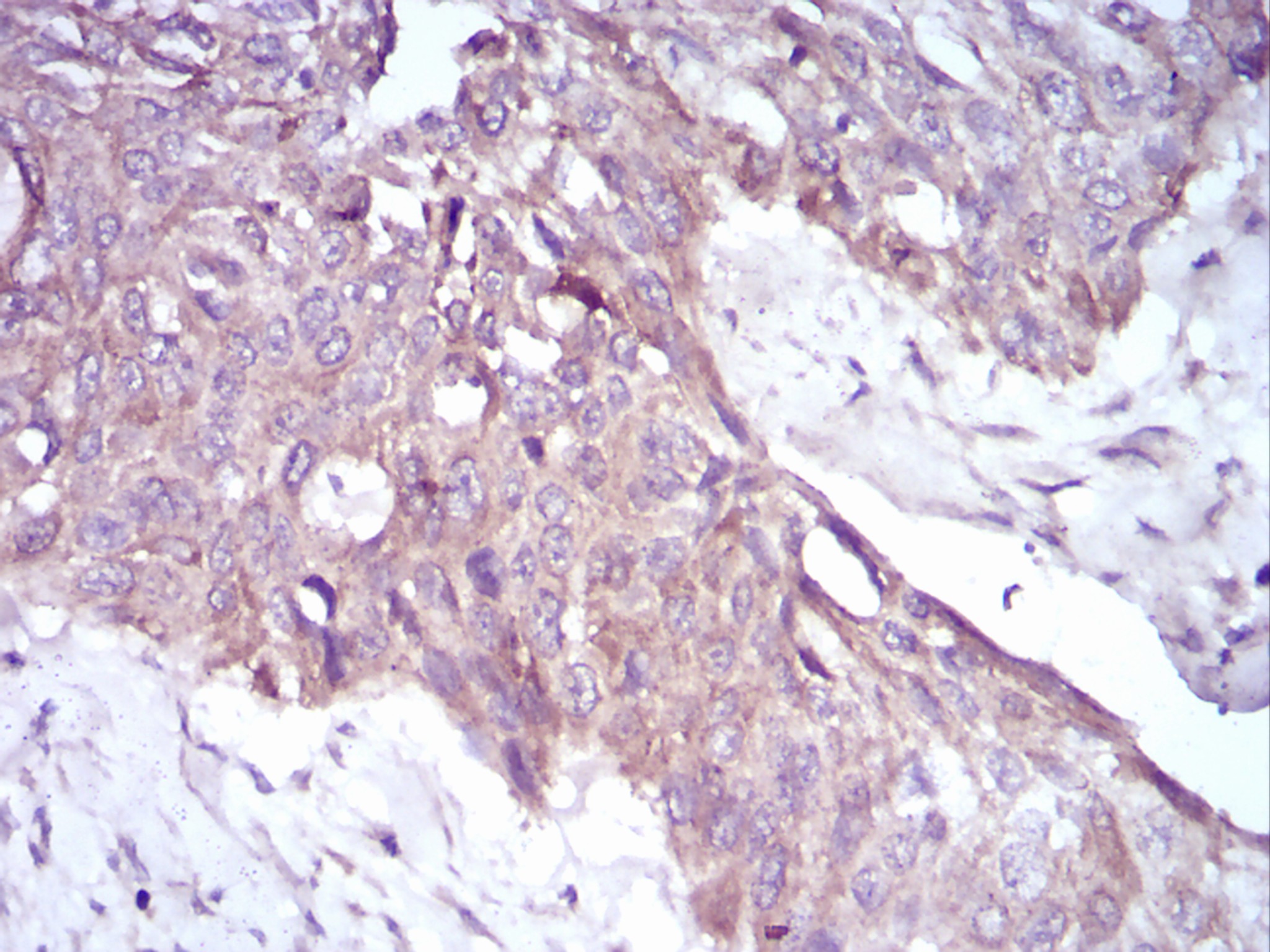
Immunohistochemical analysis of paraffin-embedded human esophageal cancer tissue using anti-PKHD1 antibody. Counter stained with hematoxylin.
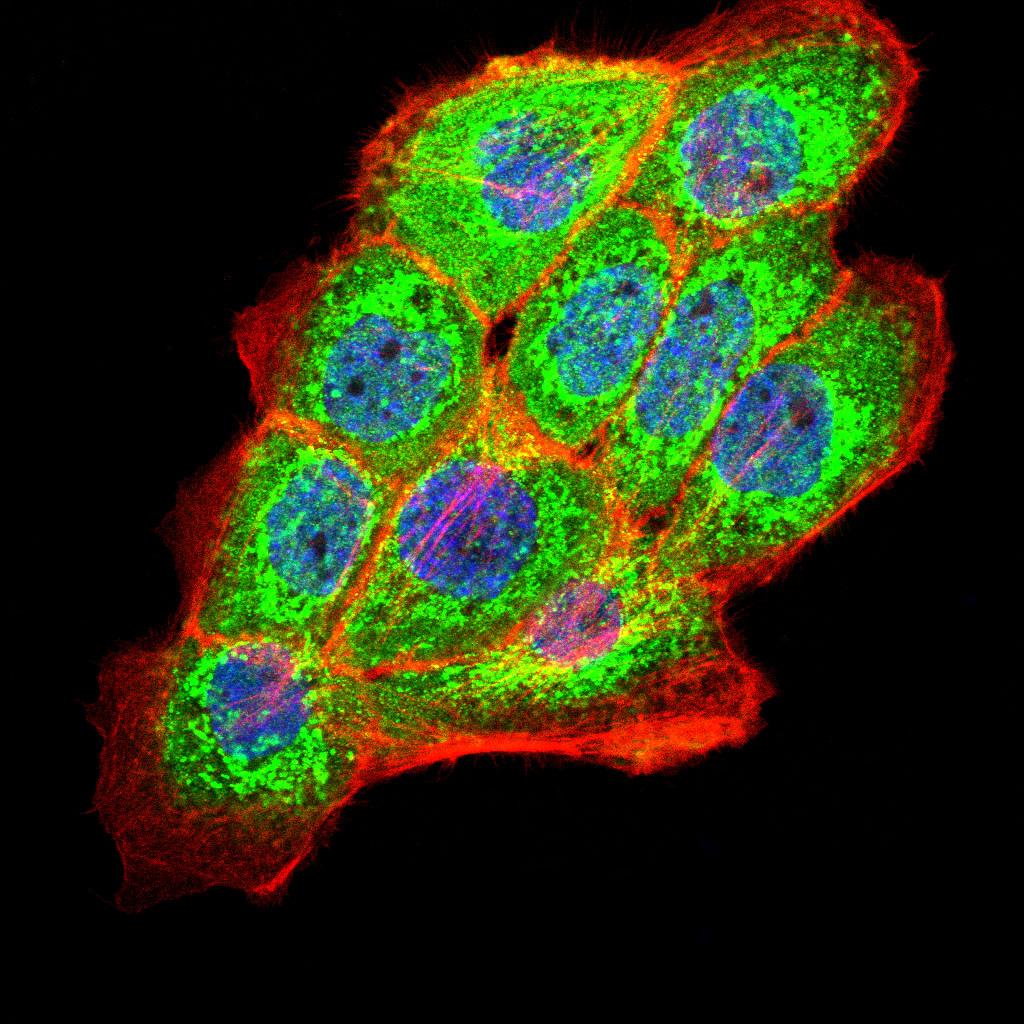
ICC staining PKHD1 (green) and Actin filaments (red) in A431 cells. The nuclear counter stain is DAPI (blue). Cells were fixed in paraformaldehyde, permeabilised with 0.25% Triton X100/PBS.
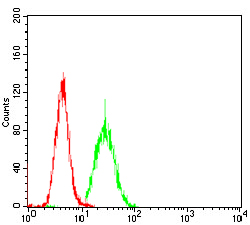
Flow cytometric analysis of Hela cells with PKHD1 antibody at 1/100 dilution (green) compared with an unlabelled control (cells without incubation with primary antibody; red).
May be required for correct bipolar cell division through the regulation of centrosome duplication and mitotic spindle assembly. May be a receptor protein that acts in collecting-duct and biliary differentiation. Defects in PKHD1 are the cause of polycystic kidney disease autosomal recessive (ARPKD). ARPKD is a severe form of polycystic kidney disease affecting the kidneys and the hepatic biliary tract. The clinical spectrum is widely variable, with most cases presenting during infancy. The fetal phenotypic features classically include enlarged and echogenic kidneys, as well as oligohydramnios secondary to a poor urine output. Up to 50% of the affected neonates die shortly after birth, as a result of severe pulmonary hypoplasia and secondary respiratory insufficiency. In the subset that survives the perinatal period, morbidity and mortality are mainly related to severe systemic hypertension, renal insufficiency, and portal hypertension due to portal-tract fibrosis.
If you have published an article using product 48398, please notify us so that we can cite your literature.

 Yes
Yes